A controversial, big-budget breast cancer screening trial that has been chronically unable to attract enough women participants since its debut in 2017 got a vote of confidence from a special working group of the National Cancer Institute (NCI) on March 17.
The Tomosynthesis Mammography Imaging Screening Trial (TMIST) should continue, but with modification, the expert group concluded in its report.
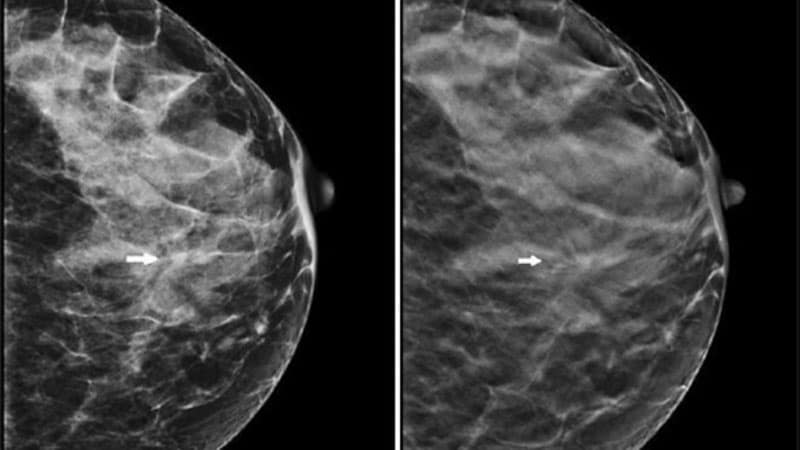
The randomized trial, with an estimated cost of $100 million, compares two kinds of mammography screenings for breast cancer in healthy women. One group of patients is screened with digital breast tomosynthesis, also known as 3-D mammography; the other is screened with the older, less expensive 2-D digital technology.
Tomosynthesis is already considered superior in detecting small cancers and reducing call backs and is increasingly being used in the real world, leading some experts in the field to say that TMIST is critically hampered by women's and radiologists' preference for 3-D mammography.
At a meeting of an NCI advisory board in September 2020, there even was a suggestion that the federal agency may kill the trial.
But at the latest meeting, the working group proposed that the trial live on.
One of the main problems with the trial has been recruitment; the recommended changes discussed at the meeting include reducing the number of women needed in the study (from 165,000 to 102,000), which would allow patient "accrual to be completed more quickly," the working group commented. In addition, the target date for completing patient accrual would be moved to 2023, 3 years after the original completion date of 2020.
The group's recommendations now go to NCI staff for scientific review. The NCI will then decide about implementing the proposed changes.
The trial, which is the NCI's largest and most expensive screening study, has never come close to targeted monthly enrollment. It was enrolling fewer than 1500 patients a month over a 2-year period, instead of the projected 5500 per month, said Philip Castle, PhD, MPH, director of the NCI's Division of Cancer Prevention, last year. He called for a review of TMIST's "feasibility and relevance" in view of the increasing use of tomosynthesis in the United States, as well as other factors.
The new technology has been "rapidly adopted" by facilities in North America, the working group noted. As of December 2020, approximately 74% of breast cancer screening clinics in the United States had at least one tomosynthesis or 3-D system; 42% of the mammography machines were 3-D.
This trend of increasing use of 3-D machines might be too much for TMIST to surmount, said Nancy Davidson, MD, of the Fred Hutchinson Cancer Research Center, in Seattle, Washington, who chaired the working group.
"We are worried the challenges [to patient accrual] may persist due to the increasing adoption of three-dimensional breast tomosynthesis in the United States over time," she commented during the working group's virtual presentation of the report to the NCI's Clinical Trials and Translational Research Advisory Committee.
Committee member Smita Bhatia, MD, PhD, of the University of Alabama at Birmingham, wondered, "What are the ongoing barriers that [TMIST investigators] are going to face beside recruitment?"
Davidson answered by speaking, again, about market penetration of tomosynthesis machines and suggested that the recruitment problems and the availability of 3-D mammography are intertwined.
"Is this a technology that has or will arrive, at which point it may not be very easy to put the genie back in the bottle?" she wondered.
That question has already been answered ― widespread use of tomosynthesis is here to stay, argues Daniel Kopans, MD, Harvard Medical School, Boston, Massachusetts, who invented digital breast tomosynthesis but no longer benefits financially from his invention because the patent has expired.
"The horse is out of the barn," Kopans told Medscape Medical News. By the time the study results are available, digital mammography will be a tool of the past, he said.
TMIST is a trial "that should never have been started in the first place, and it's failing," he said. "I was hoping they [the NCI] would say, 'Let's stop this because there's not enough accrual.' But it looks like they're not."
"TMIST is a waste of money," said Kopans, repeating a criticism he has made in the past.
A Drop in Study Power
The new recommendations for TMIST come about 1 year after Medscape Medical News reported that the study was lagging in enrollment of both patients and participating sites/physicians.
Last year, two TMIST study investigators said that it had been difficult enlisting sites, in part because many radiologists and facilities ― informed by their experience and previous research results ― already believe that the 3-D technology is superior.
Currently, most 3-D systems are used in conjunction with 2-D. First, two static images of the breast are taken (2-D), and then the unit moves in an arc, taking multiple images of the breast (3-D). Thus, 3-D is widely described as allowing clinicians to flip through the images like "pages in a book" and as offering a superior read of the breast.
The NCI working group concedes that "there is evidence that screening utilizing tomosynthesis may reduce recall rates and improve cancer detection," but it says the trial is needed to address "questions that still remain regarding the overall benefit to patients."
Furthermore, tomosynthesis "may carry higher out-of-pocket costs for women and is more labor intensive and costly for healthcare systems in that it requires about twice as much reader time for interpretation," the working group said.
The "main hypothesis of TMIST" is that "tomosynthesis will decrease the cumulative incidence of advanced breast cancers, a surrogate for mortality, compared to standard digital mammography," posits the group.
Advanced breast cancer is defined in TMIST as invasive breast cancers that meet any of the following criteria:
-
distant metastases;
-
at least one lymph node macrometastasis;
-
tumor size >1 cm and triple-negative or positive for human epidermal growth factor receptor; or
-
tumor size ≥20 mm unless of pure mucinous or other favorable histologies.
In the original study design, the study sample size was estimated to be sufficient to provide 90% power to detect a 20% relative reduction in the proportion of advanced cancers in the intervention arm (tomosynthesis, or 3-D) compared to the control arm (digital mammography, or 2-D) 4.5 years from randomization.
Now, with fewer patients and a revised analytic approach, the study's statistical power will be decreased to 80% from the original 90%.
Also, an advanced cancer is counted "if it occurs at any time while the participant is on study."
Kopans says that is a problem.
"That is a huge mistake, since digital breast tomosynthesis cannot impact prevalent cancers. They are already there. This means that their 'power calculation' is wrong, and they won't have the power that they are claiming," he comments.
Kopans explains that the first screen in TMIST will have "no effect on the number of advanced cancers." That's because the cancers will have already grown enough to become advanced, he says.
On the other hand, an initial screening might detect and thus lead to the removal of nonadvanced, smaller cancers, which, had they not been detected and removed, would have grown to become advanced cancers by the next year. Thus, the screenings done after the first year are the ones that potentially prove the effect of the intervention.
However, the working group report says that changes to the study will not affect anything other than a 10% reduction in the study's power.
The working group is concerned about TMIST going on for years and years. For that reason, they recommended that the NCI establish "strict criteria for termination of the study" if accrual goals are not met. However, those parameters have not been developed, and it was not part of the study group's mission to establish them.
The working group was sponsored by the NCI. Kopans reports consulting with DART Imaging in China.
Nick Mulcahy is an award-winning senior journalist for Medscape. He previously freelanced for HealthDay and MedPageToday and had bylines in WashingtonPost.com, MSNBC, and Yahoo. Email: nmulcahy@medscape.net and on Twitter: @MulcahyNick.
For more from Medscape Oncology, join us on Twitter and Facebook.
"breast" - Google News
March 26, 2021 at 10:23PM
https://ift.tt/3futrJ9
Huge, Struggling Breast Cancer Screening Trial Gets Lifeline - Medscape
"breast" - Google News
https://ift.tt/2ImtPYC
https://ift.tt/2Wle22m
Bagikan Berita Ini














0 Response to "Huge, Struggling Breast Cancer Screening Trial Gets Lifeline - Medscape"
Post a Comment